Why Diabesity? – There is hope for you!
Edwin J. Supit, M.D.
Internal Medicine, Functional & Lifestyle Medicine
The “New Kid” on the Block and the Unseen Driver of Modern Disease
For decades, we have been told a very specific story about our health: cut the animal fat, switch to “heart-healthy” vegetable oils, and your heart will thrive. But as a vegan physician, seeing internal medicine patients and functional medicine/lifestyle clients, I have had to face a painful reality. My own father, also a physician and a lifelong advocate of a healthy vegetarian lifestyle, succumbed to dementia during the last 15 years of his life, from age 70 to 85.
This tragedy shocked me into a 15-20-year journey of observational clinical study. I discovered that even a “clean” plant-based diet can be undermined by a silent intruder: seed oils. My father loved peanut butter, but in retrospect, I think the rapeseed and canola oils used to stabilize the specific brand he consumed daily likely played a significant role in his clinical outcome. Today, as a pragmatist, I observe daily with my hundreds and thousands of patients dramatic clinical improvements—from hypertension, diabetes, and obesity to cognitive function, arthritis, and many chronic inflammations—not by counting calories, but by removing these industrial oils and returning to the biological wisdom of traditional fats like coconut oil.
The Heart of the Matter: A Historical Shift
In the 1930s, cardiologists made up less than 1% of the medical profession. Why? Because coronary artery disease and “blocked arteries” simply weren’t the main story of the day. Fact: Myocardial infarction (heart attack) was considered a clinical rarity.
- The Vanishing Baseline: In Indonesia, the Philippines, and Guam, obesity was nearly non-existent before the 1940s. It remained low until the 1980s, when the “vilification” of saturated fats and cholesterol led to a massive influx of stabilized, unsaturated seed oils.
- The Guam Reality: Today, we see patients reverse their weight and diabetes without cutting back their traditional rice. Their “secret” is simply avoiding the hidden seed oils—canola, soy, corn, sesame, and even avocado or olive oils—found as a minute addition in everything from dressings and mayo to granola bars and commercial mixed nuts.
The Mechanism: Jamming the Cellular Doors
This “Diabesity” epidemic is not about sugar. It is about a catastrophic imbalance in essential fatty acids. Your 30 trillion cells each have a “door” (the cell membrane) and a “doorbell” (the insulin receptor). The problem we see is an extreme overpowerment of proinflammatory Omega-6 unsaturated fats over the “good,” lubricating anti-inflammatory Omega-3 fats.
Omega-3s help “lubricate” the cell doorbells and allow sugars from the blood stream to enter the cells, while driving down conditions like arthritis and pain. In contrast, the unstable seed oils lead to membrane phospholipid replacement, creating “sticky” and “stiff” cell walls.
The results are stark:
| Insulin Metric | Healthy State | Seed Oil State |
| Pancreatic Insulin Release | Only 5 IU | Hours/days of high insulin levels |
| Cellular Response | “Doorbells” open instantly | “Cell doors don’t readily open, starving cells” |
| Blood Sugar Clearance | Cleared in minutes | Stays in blood for hours/days |
| Blood Sugar Level | <100 mg/dL under 2 hours | 126–300+ mg/dL even after 24 hours |
The 680-Day Problem: Why Your Body Can’t “Forget” Seed Oils
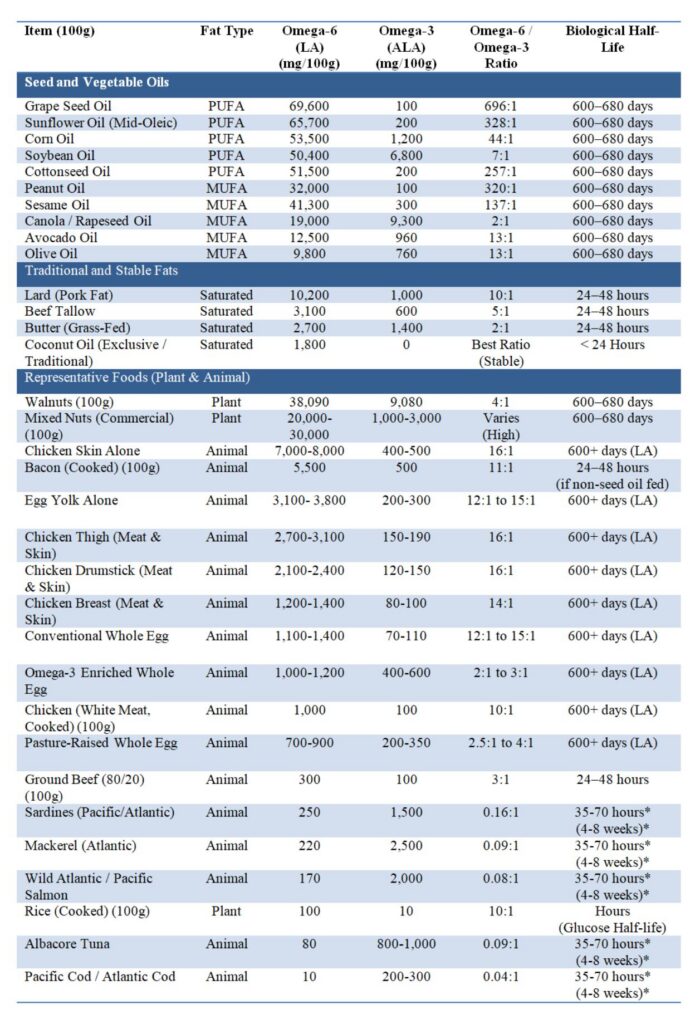
Traditional saturated fats (butter, beef tallow, coconut oil) are rapidly processed from the blood by the liver in 24–48 hours. Modern seed oils stick around (~1-2 years) and are incorporated into your adipose (fat) tissue, many cell membranes, including mitochondrial membranes, where they cause cumulative damage, chronic inflammation, metabolic syndrome, endothelial nitric oxide suppression, mitochondrial respiratory chain dysfunction and energy transport disruption. To understand the root cause of the modern epidemic, we must look at the data.
In this table, I have provided factual evidence of the differences which can help elucidate the historical and biochemical reasons for the epidemic that has transpired since the 1940s. Note the biological half-lives (how long the fats stay in the blood or in the tissue membranes).
Data of Common Fats and Representative Foods
(A partial list, sorted by descending Omega-6 content per category)
- Biological Half-Life of (EPA/DHA, the “good”) omega-3 fats in Humans
- Acute Plasma Clearance *(Circulating Half-Life):
- EPA (Eicosapentaenoic Acid): ~35 – 45 hours in blood plasma following ingestion.
- DHA (Docosahexaenoic Acid): ~60 – 70 hours in blood plasma.
- Tissue Integration & Elimination *(Membrane Half-Life):
- Once incorporated into cell membranes (e.g., red blood cells, cardiac tissue, neural tissue), long-chain omega-3 fatty acids turnover much more slowly.
- The erythrocyte (RBC) membrane half-life of EPA/DHA is approximately 4 to 8 weeks (requiring 3–4 months of consistent intake to reach steady-state saturation across systemic tissue stores).
- Acute Plasma Clearance *(Circulating Half-Life):
- Highlighting Coconut Oil’s Advantage: As shown above, coconut oil and its Medium Chain Triglycerides (MCT) have the lowest proinflammatory Omega-6 content (just 1.8g per 100g) and the fastest biological clearance (<24 hours). This unique, stable fat promoted the profound metabolic and cardiovascular health of many Pacific islanders for centuries before seed oils were introduced.
- In looking at the chart, consider :
- the total omega-6 fat content (in general you want this low),
- the total omega-3 fat content (in general you want this high),
- the ratio of omega-6 to omega-3 oils (a 4:1 ratio or less is ideal),
- and choose the lowest biological half-life of the omega-6 oils (how long it stays in your cells, the lowest is ideal);
- and choose the longer cellular half-life of omega-3 oils (how long it stays in your cells, the longer is ideal for omega-3, anti-inflammatory fats).
The Turning Point: Clinical Wins
When patients shift exclusively to stable fats like unodorized coconut oil for cooking, without “calorie restriction” or calorie counting, the cellular carbs stop “starving.” When combined with a whole foods, predominantly unrefined plant-based nutritional lifestyle (avoiding stimulants like caffeine, soda or alcohol) coupled with moderate exercise, patients simply achieve the best of their clinical outcome (diabetes, hypertension,obesity, chronic arthritis, heart failure, etc.), many within 1-2 months while enjoying each meal to satisfaction without much worrying about strict carbs-restriction in general.
- Heart Failure Recovery: Patients see proBNP levels dramatically improve, allowing many to come off medications without leg swelling or fluid in the lungs as early as 1–2 months or less.
Conclusion
The path forward is clear: changing the quality of our fats is key. By minimizing our Omega-6 “baggage” and restoring our cellular “lubrication,” we can finally make progress against diabesity and chronic disease,especially in Guam, USA and everywhere.
See further scientific evidence in the supplied research papers below.
Scientific References & Citations
White Paper Content & Professional References:
- Beynen, A. C., et al. (1980). “Composition of adipose tissue in relation to saturated and polyunsaturated fat intake.” CRC Critical Reviews in Food Science and Nutrition. (Documentation of linoleic acid half-life and tissue retention).
- Dayton, S., et al. (1966). “Composition of lipids in human serum and adipose tissue during prolonged feeding of a diet high in unsaturated fat.” Journal of Lipid Research. (Evidence for the 600–680 day biological half-life of PUFAs).
- Dinan, T. G., et al. (2011). Omega-6 to Omega-3 Fatty Acid Ratio and Inflammation. Clinical Nutrition. (Mechanism of inflammation and cellular signaling).
- Knapp, H. R., & Fitzgerald, G. A. (1989). The antihypertensive effects of fish oil. New England Journal of Medicine. (Effect of balancing fats).
- Prior, I. A., et al. (1981). “Cholesterol, coconuts, and diet on Polynesian islands: a natural experiment.” The American Journal of Clinical Nutrition. (Evidence of historical health and coconut consumption).
- Sircar, S., & Kansra, U. (1998). Choice of cooking oils—myths and realities. Journal of Indian Medical Association. (Historical medical data of early 20th century).
- White, P. D. (1931). Heart Disease. MacMillan. (Cardiology data before 1930).
- Yamashima, T. (2012). Reevaluating the ‘Vegetable Oil’ Theory of Alzheimer’s Disease. Progress in Lipid Research. (Regarding Rapeseed/Canola oil and neural death).
Factual Evidence on Nutrient Composition (Nutritional Tables):
- Guasch-Ferré, M., et al. (2015). “Olive oil consumption and risk of cardiovascular disease and all-cause mortality: A systematic review and meta-analysis.” American Journal of Clinical Nutrition. (Olive/Avocado Omega-6/MUFA profile).
- United States Department of Agriculture (USDA). (2023). FoodData Central. (Source for fatty acid composition data of all oils and representative foods).
Share this as PDF file:
![]()