TABLE OF CONTENTS
I. Comprehensive Review: Functional Medicine Mechanisms
- Part 1: Foundational Mechanisms of Dysautonomia (Autoimmune, Neuropathic, and Sympathetic Factors)
- Part 2: The Functional Medicine “Perfect Storm” (Micronutrient & Mineral Deficiencies)
- Part 3: The Central Cofactor Axis (Copper, Vitamin C, and Catecholamine Enzyme Dysfunction)
II. Laboratory Analytes for Dysautonomia
- A Root-Cause Assessment Guide
III. Recovery Protocol
- A Whole-Food, Vegan, and Lifestyle Protocol for Dysautonomia Recovery
If you are struggling with dysautonomia, also known as Postural Orthostatic Tachycardia Syndrome (POTS), this article provides some insights from a functional medicine, lifestyle and nutritional perspective to help you in your search and recovery of health.
Comprehensive Review:
Functional Medicine Mechanisms of Dysautonomia with a Focus on Caffeine, Copper Dysregulation, Adrenal Function, and Nutritional Imbalances
This document synthesizes the mechanisms of dysautonomia from a functional medicine perspective, integrating the roles of micronutrient deficiencies, caffeine, copper dysregulation, vitamin C-dependent adrenal function, and dietary triggers.
Part 1: Foundational Mechanisms of Dysautonomia
Dysautonomia refers to a group of conditions resulting from malfunction of the autonomic nervous system (ANS). The ANS regulates involuntary functions like heart rate, blood pressure, digestion, and temperature control. Mechanistically, it is not one disease but a spectrum of disorders with overlapping pathophysiologies (Saperstein et al., 2020).
1.1 Autoimmune and Inflammatory Basis
A significant subset of dysautonomia, particularly Postural Orthostatic Tachycardia Syndrome (POTS), is now understood to have an autoimmune etiology. Autoantibodies, often targeting G-protein coupled receptors (GPCRs) such as adrenergic and muscarinic receptors, act as either agonists or antagonists, disrupting normal ANS signaling. Cross-reactivity following a viral infection is a common triggering event. Inflammatory cytokines can directly impair the function of the baroreflex and increase sympathetic outflow at the central nervous system level.
1.2 Neuropathic and Connective Tissue Factors
A length-dependent autonomic neuropathy, often a small fiber neuropathy, damages the vasomotor nerves in the lower extremities. This causes venous pooling and a compensatory, excessive sympathetic activation upon standing. A strong association exists between Ehlers-Danlos Syndrome (EDS) and dysautonomia, where abnormal collagen leads to increased vascular distensibility and venous pooling.
1.3 Sympathetic Overactivity and Hypovolemia
Many patients have a hyperadrenergic state characterized by elevated norepinephrine levels, either as a primary condition or secondary to neuropathy and hypovolemia. Inappropriately low plasma renin and aldosterone levels can lead to profound hypovolemia, further driving a reflex tachycardia to maintain cardiac output.
Part 2: The Functional Medicine “Perfect Storm”: Micronutrient & Mineral Deficiencies
Functional medicine views dysautonomia as a system-wide breakdown where nutritional deficiencies are primary drivers of ANS instability, often acting as the “perfect storm” alongside genetic predisposition and environmental triggers.
2.1 Vitamin B12 and Methylation
A deficiency in B12 can cause autonomic dysfunction through demyelination of autonomic nerves. Functionally, even low-normal serum levels may be inadequate, requiring assessment of methylmalonic acid and homocysteine. Impaired methylation due to B12 or folate deficiency disrupts the synthesis of catecholamines and their degrading enzymes (COMT) (Saperstein et al., 2020).
2.2 Vitamin D
Vitamin D receptors are present in the ANS and regulate nerve growth factor. Deficiency is linked to increased sympathetic tone and blunted parasympathetic recovery. It also modulates the immune system, potentially reducing the production of GPCR autoantibodies (Wimalawansa, 2019).
2.3 Iron (Ferritin)
A ferritin level below 50 µg/L can exacerbate tachycardia and fatigue, even without anemia. Iron is a cofactor for tyrosine hydroxylase, the rate-limiting enzyme in norepinephrine synthesis. Low iron impairs thermoregulation, a key autonomic function (Jarjour & Jarjour, 2013).
2.4 Magnesium
This mineral is a physiological calcium channel blocker and NMDA receptor antagonist. Deficiency creates a state of sympathetic hyperarousal, vasospasm, and poor cardiac diastolic relaxation. It is crucial for parasympathetic nerve function via the vagus nerve (Sartori et al., 2012).
Part 3: The Central Cofactor Axis: Copper, Vitamin C, and Catecholamine Enzyme Dysfunction
This section details the critical biochemical intersection of copper, vitamin C, and caffeine. These factors converge on a single, pivotal enzyme system—dopamine-β-hydroxylase (DBH)—and adrenal function, making their combined dysregulation a central driver of ANS instability.
3.1 The Dopamine-β-Hydroxylase (DBH) Bottleneck: A Two-Cofactor System
DBH is the enzyme responsible for converting dopamine to norepinephrine within sympathetic nerve vesicles and the adrenal medulla. Its function is uniquely dependent on two cofactors working in concert: copper as the catalytic metal, and ascorbate (vitamin C) as the specific, obligate electron donor for the hydroxylation reaction (Levine et al., 1996). A deficiency in either creates a functional bottleneck with identical clinical consequences: elevated dopamine, impaired norepinephrine synthesis, compensatory adrenergic receptor hypersensitivity, and an unstable hyperadrenergic state. This dual dependency is a cornerstone of the functional medicine model, as it explains why addressing only one deficiency while neglecting the other often fails to resolve symptoms.
3.2 Mechanisms of Caffeine-Induced Copper Dysregulation
Caffeine and its metabolites influence copper homeostasis at two primary levels, creating a functional copper deficiency that can occur even with “normal” dietary intake and serum levels (Kumar, 2006).
- Chelation and Absorption Blockade: Caffeine, along with related methylxanthines found in coffee and tea, is a known chelator of divalent cations. It forms complexes with copper in the gastrointestinal tract, directly inhibiting its absorption. Chronic caffeine consumption can significantly reduce copper status in tissues, including the heart and liver.
- Exaggerated Biliary Excretion: Caffeine stimulates the hepatic production of metallothionein, a cysteine-rich protein that tightly binds copper. This copper-metallothionein complex is then preferentially excreted into the bile. This mechanism diverts copper away from its essential destination, which is incorporation into ceruloplasmin and other cuproenzymes, and instead shunts it for elimination. This is the same pathway by which high-dose zinc induces copper deficiency, highlighting that caffeine can mimic this well-known functional root cause.
The result is a copper-deficient state within the tissues, particularly the nervous and cardiovascular systems, which is not always reflected by a low serum copper or ceruloplasmin test because the body maintains circulating levels at the expense of tissue stores.
3.3 The Role of Vitamin C and Adrenal Function in Dysautonomia
Vitamin C (ascorbic acid) is concentrated at remarkably high levels in the adrenal glands, where it plays two distinct and indispensable roles: one in the adrenal medulla for catecholamine synthesis, and the other in the adrenal cortex for steroidogenesis and antioxidant protection (Padayatty et al., 2003).
- Vitamin C as a DBH Cofactor: As detailed above, without adequate intravesicular ascorbate, DBH activity is rate-limited regardless of copper status. The adrenal medulla’s demand for ascorbate is so high that it is one of the first tissues to be depleted under physiological stress (Levine et al., 1996).
- Vitamin C, Cortisol, and the Adrenal Cortex: The adrenal cortex requires vitamin C for cortisol synthesis and for protecting itself from oxidative damage. Vitamin C is a necessary cofactor for several cytochrome P450 enzymes involved in converting cholesterol to cortisol. During ACTH stimulation, ascorbate is released from the cortex alongside cortisol. Furthermore, cortisol synthesis generates a high flux of reactive oxygen species (ROS); the cortex accumulates millimolar concentrations of ascorbate to quench these ROS, preventing autolysis of the gland (Patak et al., 2004).
- The Vicious Cycle in Dysautonomia: In a state of chronic sympathetic overactivity, the relentless demand for cortisol and catecholamines depletes adrenal ascorbate stores. A depleted adrenal gland cannot efficiently produce cortisol, impairing the body’s ability to regulate inflammation, maintain vascular tone, and respond to hemodynamic stress. This functional adrenal insufficiency clinically presents as extreme fatigue, salt-wasting (from relative aldosterone deficiency), and worsening orthostatic intolerance. The patient exhibits a hyperadrenergic state that paradoxically “crashes,” a pattern identified by Marik (2020) as driven by the rapid depletion of this essential “stress hormone.” Replenishing vitamin C is a foundational strategy to restore both DBH and P450 enzyme function, thereby stabilizing the autonomic response (Marik, 2020).
3.4 Copper-Related Enzyme Dysfunction Beyond DBH
Beyond the DBH bottleneck, copper deficiency from caffeine disrupts other critical enzymes that directly manifest as dysautonomia symptoms.
- Peptidylglycine α-Amidating Monooxygenase (PAM): The Neuropeptide Connection
PAM is another copper-dependent enzyme required for the activation of numerous neuropeptides via C-terminal amidation. PAM dysfunction renders key peptides inert: Vasoactive Intestinal Peptide (VIP, impairing vagal tone), Cholecystokinin (CCK, causing digestive symptoms), and Neuropeptide Y (NPY, contributing to blood pressure instability) (Bousquet-Moore et al., 2010). - Cytochrome c Oxidase (COX): The Mitochondrial Energy Connection
COX is Complex IV of the mitochondrial electron transport chain, the final, copper-containing enzyme that drives ATP synthesis. Autonomic nerves have extremely high metabolic demands. Impaired COX activity from copper deficiency creates an energy deficit manifesting as axonal transport failure and “cardiac pacing exhaustion,” mimicking a “tired heart” rhythm disturbance (Matoba et al., 2005). - Lysyl Oxidase (LO): The Connective Tissue Connection
This secreted copper-dependent enzyme cross-links collagen and elastin, providing tensile strength to blood vessels and nerve epineurium. LO dysfunction results in weakened, hyper-distensible blood vessels, exacerbating venous pooling in the lower extremities—the primary mechanical trigger of POTS. This is a key mechanism in the overlap with Hypermobility Spectrum Disorders, representing an acquired vascular laxity from caffeine-induced copper deficiency (Smith-Mungo & Kagan, 1998).
Part 4: Dietary Triggers of Autonomic Instability
4.1 Caffeine: A Vasopressor and Sympathetic Amplifier
Caffeine’s effect in dysautonomia is highly individualized and mechanistically paradoxical, beyond its impact on copper homeostasis (Benowitz, 1990).
- Vasopressor and Volume Shifting: As an adenosine receptor antagonist, caffeine is a potent vasoconstrictor. For patients with neuropathic POTS and venous pooling, this can improve venous return and reduce reflex tachycardia. This is the basis for its pharmacological use in some vasovagal syncope protocols.
- Sympathetic Amplifier and Diuretic: In hyperadrenergic POTS, caffeine synergizes with elevated norepinephrine, causing a potentially dangerous increase in heart rate, anxiety, and tremors. Its diuretic effect can also worsen the hypovolemia that underpins many POTS cases. Mechanistically, it increases sympathetic burst frequency directly through central stimulation (Benowitz, 1990).
4.2 Low Carbohydrate Diets and Hypovolemia
A low-carbohydrate or ketogenic diet can be profoundly destabilizing due to the renal handling of sodium (Borer, 2013).
- The Insulin-Kidney Axis: Insulin promotes sodium reabsorption in the proximal renal tubules. A low-carbohydrate intake lowers circulating insulin levels, signaling the kidneys to waste sodium (natriuresis). For a person already prone to hypovolemia, this natriuretic effect can cause a severe drop in plasma volume.
- Glycogen Depletion: Each gram of glycogen is stored with approximately 3-4 grams of water. Depleting glycogen stores can cause a rapid loss of 2-5 pounds of water weight, directly reducing blood volume and exacerbating tachycardia.
- Physiological Insulin Resistance and Norepinephrine: To preserve glucose for the brain, a prolonged low-carb diet increases sympathetic nervous system activity and circulating norepinephrine to promote lipolysis and hepatic gluconeogenesis. In hyperadrenergic patients, this dietary state mimics their disease state (Borer, 2013).
4.3 Seed Oils, Omega-6 Imbalance, and Neuropathic Inflammation
The high intake of linoleic acid (LA) from industrial seed oils and its oxidized metabolites drives a pro-inflammatory state targeting small nerve fibers (DiNicolantonio & O’Keefe, 2018).
- Pro-Inflammatory Eicosanoids: An elevated omega-6:3 ratio shifts the lipid mediator profile towards the synthesis of inflammatory prostaglandins and leukotrienes, fueling chronic, low-grade inflammation.
- Oxidative Stress and Small Fiber Neuropathy: The polyunsaturated fats in seed oils are highly susceptible to lipid peroxidation, especially when heated. Resulting reactive aldehydes, like 4-hydroxynonenal (4-HNE), are directly neurotoxic, damaging mitochondrial membranes in dorsal root ganglia and contributing to the small fiber neuropathy that often underlies dysautonomia (DiNicolantonio & O’Keefe, 2018).
Part 5: The Functional Medicine Synthesis: The Caffeine-Copper-Vitamin C “Vicious Cycle”
The clinical picture from a functional medicine perspective is a cascading, self-reinforcing loop:
- A patient with a stressful lifestyle (high sympathetic tone) uses caffeine for energy.
- Caffeine acutely worsens GI motility and absorption while increasing biliary copper excretion (Kumar, 2006).
- The resulting functional copper deficiency, combined with chronic stress-induced depletion of adrenal ascorbate, creates a dual hit on DBH function. This leads to unstable norepinephrine synthesis and a hyperadrenergic state that worsens the original fatigue and anxiety (Prohaska & Broderius, 1997; Levine et al., 1996).
- Simultaneously, impaired PAM, COX, and adrenal cortical function degrade parasympathetic (vagal) tone, mitochondrial energy, and the capacity to produce cortisol for hemodynamic stability, leading to gastroparesis, profound exhaustion, and orthostatic intolerance (Bousquet-Moore et al., 2010; Matoba et al., 2005; Marik, 2020).
- The patient, feeling worse, consumes more caffeine to self-medicate the very symptoms the caffeine is driving, further depleting copper and vitamin C.
This pattern is often missed on standard labs. Functional medicine assessment focuses on recognizing the pattern: a hyperadrenergic, hypermobile patient with high caffeine intake and signs of adrenal dysfunction, requiring a comprehensive strategy of caffeine cessation, copper repletion, and high-dose vitamin C to break the cycle and restore DBH, PAM, COX, LO, and adrenal cortical function.
Summary Table of Mechanisms
| Factor | Functional Medicine Mechanism | Key Biochemical Pathway | Key Reference(s) |
|---|---|---|---|
| Micronutrient Deficiencies | Cofactor depletion for enzyme function (e.g., B12 for methylation, Mg for NMDA). | Impaired catecholamine synthesis & degradation; CNS hyperarousal. | Saperstein et al., 2020; Sartori et al., 2012 |
| Caffeine, Copper & Vitamin C Axis | Chelation & biliary Cu excretion; stress-induced Vit C depletion; dual DBH cofactor failure. | ↓ DBH activity -> unstable norepinephrine; ↓ PAM -> inert neuropeptides; ↓ COX -> mitochondrial failure; ↓ Cortisol -> hemodynamic instability. | Prohaska & Broderius, 1997; Levine et al., 1996; Bousquet-Moore et al., 2010; Matoba et al., 2005; Marik, 2020 |
| Low Carbohydrate Diet | Dietary-induced natriuresis and glycogen-associated water loss. | Low insulin -> impaired renal sodium reabsorption -> hypovolemia -> reflex SNS activation. | Borer, 2013 |
| Omega-6 (Seed Oils) | Chronic substrate for neurotoxic lipid peroxidation. | Linoleic acid -> Oxidized LDL & 4-HNE -> mitochondrial damage in small nerve fibers -> neuropathy. | DiNicolantonio & O’Keefe, 2018 |

The following is a comprehensive guide to functional medicine laboratory analytes for dysautonomia, logically organized by physiological system. This panel goes far beyond standard conventional labs to assess the root biochemical drivers detailed in the preceding documents: micronutrient status, copper-vitamin C-DBH axis function, adrenal health, mast cell activation, autoimmunity, and energy metabolism.
II. Functional Medicine Laboratory Analytes for Dysautonomia: A Root-Cause Assessment Guide
This panel is designed to investigate the “perfect storm” of mechanisms driving autonomic instability, moving beyond diagnosis to identify actionable, personalized therapeutic targets.
Part 1: Copper, Zinc, and Ceruloplasmin Axis (The DBH and PAM Cofactor Status)
This is the highest-priority assessment to identify the functional copper deficiency caused by caffeine, high-dose zinc supplementation, or malabsorption, which impairs DBH, PAM, COX, and LO (Prohaska & Broderius, 1997; Bousquet-Moore et al., 2010).
- Serum Copper: Measures total circulating copper. A low level confirms frank deficiency. However, a normal or high level does not rule out a functional deficiency, as inflammation raises serum copper and ceruloplasmin.
- Serum Ceruloplasmin: The primary copper-binding protein. This is an acute-phase reactant, so it must be interpreted alongside inflammatory markers (hs-CRP). If ceruloplasmin is low, it strongly suggests copper deficiency (Kumar, 2006).
- Serum Zinc: Must be ordered simultaneously. Zinc and copper compete for absorption. A high-normal or high zinc level (often from supplementation) is a classic cause of copper deficiency. The ideal zinc:copper ratio is approximately 0.8–1.2.
- Calculated Free Copper: This is a calculation, not a direct test: Free Copper (µg/dL) = Total Serum Copper (µg/dL) – [Ceruloplasmin (mg/dL) x 3.15]. It estimates the unbound, bioactive copper pool and can be elevated in states of oxidative stress and inflammation.
- 24-Hour Urinary Copper: Useful to rule out Wilson’s disease if free copper is very high, or to assess excessive renal excretion as a cause of deficiency.
Part 2: Adrenal and Catecholamine Assessment (The Vitamin C-DBH-Adrenal Axis)
This panel evaluates the functional consequences of vitamin C depletion and the hyperadrenergic/hypocortisol state driven by chronic stress and caffeine (Levine et al., 1996; Marik, 2020; Patak et al., 2004).
- 4-Point Dried Urinary Cortisol and Cortisone (Diurnal Rhythm): This is a cornerstone assessment. It maps the circadian secretion of free cortisol. A typical dysautonomia pattern shows a low-morning “flatlining” cortisol profile (adrenal insufficiency/fatigue from chronic overstimulation and Vitamin C depletion) with potential evening spikes. It also provides the cortisol-to-cortisone ratio, assessing 11β-HSD enzyme activity.
- DHEA-S (Serum): An adrenal androgen that often declines with chronic stress. A low level supports adrenal insufficiency and poor resilience.
- Plasma or Fractionated Urinary Catecholamines (Norepinephrine, Epinephrine, Dopamine):
- Supine and Standing Plasma Catecholamines: The diagnostic test for hyperadrenergic POTS. A norepinephrine level >600 pg/mL upon standing is the classic cutoff.
- Functional Perspective: A high dopamine relative to norepinephrine suggests a DBH bottleneck (functional copper or vitamin C deficiency) where the conversion is rate-limited. This pattern is a key clinical clue.
Part 3: Volume Status and Electrolyte Regulation (The RAAS and Hypovolemia Axis)
These tests clarify the drivers of hypovolemia, a central mechanism in POTS.
- Renin Activity (Plasma Renin Activity or Direct Renin): In hypovolemic POTS, renin is often inappropriately low-normal or low despite obvious signs of volume depletion. This is a paradoxical finding that distinguishes the condition from simple dehydration.
- Aldosterone (Serum): Similarly, aldosterone may be inappropriately low relative to the renin level and the clinical state of hypovolemia, explaining the body’s inability to retain sodium effectively.
- Comprehensive Metabolic Panel (CMP): Standard electrolytes (sodium, potassium, chloride, CO2). Must be viewed functionally; a low-normal CO2 (bicarbonate) can indicate chronic, compensated respiratory alkalosis from hyperventilation, a common feature.
- Serum and Urine Osmolality: Used to assess antidiuretic hormone (ADH) axis function and the kidney’s ability to concentrate urine, ruling out diabetes insipidus.
Part 4: Micronutrient Status (The “Perfect Storm” Cofactors)
Directly assesses the key vitamin and mineral deficiencies implicated in autonomic neuropathy and hyperreactivity.
- Vitamin B12 & Folate: Serum levels are insufficient. Must also test Methylmalonic Acid (MMA) and Homocysteine. Elevated MMA is a more sensitive and specific marker for functional B12 deficiency at the tissue level, which causes autonomic demyelination (Saperstein et al., 2020).
- Ferritin & Iron Panel: Aim for a ferritin >50 µg/L. Low iron is a cofactor deficiency for tyrosine hydroxylase, the rate-limiting enzyme for norepinephrine synthesis, and impairs thermoregulation (Jarjour & Jarjour, 2013).
- Magnesium (RBC): Red blood cell magnesium is a better indicator of long-term tissue status than serum magnesium. Deficiency drives sympathetic hyperarousal (Sartori et al., 2012).
- Vitamin D (25-OH): Optimal levels (50-80 ng/mL) are needed for ANS regulation and immune modulation to reduce GPCR autoantibody production (Wimalawansa, 2019).
Part 5: Inflammatory and Autoimmune Drivers
These assess the autoimmune and mast cell components often at the root of the condition.
- High-Sensitivity C-Reactive Protein (hs-CRP): A measure of systemic inflammation. Important to interpret alongside ceruloplasmin.
- Tryptase (Serum): A screening test for Mast Cell Activation Syndrome (MCAS), a frequent comorbidity. MCAS drives paroxysmal sympathetic activation and vasodilation.
- Plasma Histamine and 24-Hour Urinary N-Methylhistamine: More specific markers of mast cell burden.
- Autoantibody Testing (Cell-Based Assays): Specialized testing available through functional medicine labs (e.g., CellTrend, Mayo Clinic) for GPCR autoantibodies:
- Alpha-1 Adrenergic Receptor
- Beta-1 and Beta-2 Adrenergic Receptors
- Muscarinic Cholinergic Receptor (M1, M2)
- Angiotensin II Type 1 Receptor
Part 6: Gastrointestinal and Nutritional Absorption Assessment
Since dysautonomia causes gastroparesis and altered motility, nutrient malabsorption is a key root cause.
- Comprehensive Stool Analysis: Assesses digestion, absorption, pancreatic elastase (often low in vagal dysfunction), gut inflammation, and microbiome balance. This reveals why oral nutrient replacement may be failing.
- Leaky Gut Markers: Serum zonulin or fecal calprotectin/secretory IgA can indicate intestinal permeability, a driver of systemic inflammation and autoimmunity.
Summary Table of Analytes and Target Mechanisms
| Category | Key Analytes | Target Mechanism |
|---|---|---|
| Copper Axis | Serum Cu, Ceruloplasmin, Zn, Free Cu | Rate-limiting cofactor for DBH, PAM, COX, LO. |
| Adrenal Axis | 4-Point DUTCH (Cortisol, Cortisone), DHEA-S, Catecholamines | Vitamin C-dependent catecholamine/cortisol synthesis; hyperadrenergic state. |
| Volume/RAAS Axis | Renin, Aldosterone, CMP, Osmolality | Hypovolemia; inappropriate sodium wasting; paradoxical RAAS blunting. |
| Micronutrients | MMA, Homocysteine, Ferritin, RBC Mg, 25-OH Vit D | Nerve myelination; cofactors for catecholamine synthesis and autonomic stability. |
| Inflammation/Autoimmunity | hs-CRP, Tryptase, GPCR Autoantibodies | Autoimmune receptor disruption; mast cell-driven autonomic instability. |
| Gut Function | Stool Analysis (Elastase, Calprotectin), Zonulin | Malabsorption driving micronutrient deficiencies; leaky gut driving autoimmunity. |
This panel provides a comprehensive physiological map, enabling a precise, personalized protocol that targets the specific deficiencies, toxicities, and imbalances driving an individual’s dysautonomia.

The following is a comprehensive protocol to help in your healing journey.
III. A Whole-Food, Vegan, and Lifestyle Protocol for Dysautonomia Recovery: Emphasizing Carbohydrates for Cellular Energy
This protocol translates the identified mechanisms—copper-vitamin C-DBH axis failure, micronutrient deficiencies, hypovolemia, mitochondrial dysfunction, and neuro-inflammation—into actionable, natural, and vegan strategies. A central emphasis is placed on the indispensable role of carbohydrates for autonomic cellular energy efficiency, countering the destabilizing effects of low-carb diets.
Part 1: The Absolute Priority – Eliminating Inflammatory and Controversial Triggers
Before the nervous system can heal, the primary drivers of neuro-inflammation and autonomic instability must be removed. This step is non-negotiable.
1.1 Strict Avoidance of All Seed Oils and Controversial Extracted Oils
This is the single most important dietary change for reducing the neuropathic inflammation that underlies many forms of dysautonomia. Industrial seed oils are the concentrated source of linoleic acid (LA), the omega-6 fat that fuels a pro-inflammatory cascade and directly damages small nerve fibers (DiNicolantonio & O’Keefe, 2018). Due to ongoing controversies, this protocol also excludes all other extracted oils, focusing solely on whole-food fats and coconut oil.
- Oils to Avoid Completely:
- Industrial Seed Oils: Soybean oil, corn oil, sunflower oil, safflower oil, canola oil, cottonseed oil, grapeseed oil, and rice bran oil.
- Controversial Fruit Oils (Excluded in this Protocol): Olive oil, avocado oil.
- Other Extracted Nut/Seed Oils: Sesame oil, walnut oil, flaxseed oil.
- The “Whole-Food Fats Only” Rule: All dietary fat must come from intact whole foods (avocados, olives, nuts, seeds, coconut) or from coconut oil, which is permitted as the sole extracted oil.
- Practical Elimination Steps: Read every label; assume restaurant food contains these oils unless verified otherwise; overhaul the home pantry to an extracted-oil-free zone with the single exception of coconut oil.
1.2 Caffeine Elimination and Gradual Weaning
This is the second critical elimination to halt the caffeine-induced copper depletion and sympathetic amplification (Benowitz, 1990; Kumar, 2006). The structured weaning protocol transitions from coffee to caffeine-free natural juices rich in vitamin C and magnesium for adrenal support during withdrawal, reducing intake by 25% every 3-4 days over 2-3 weeks.
Part 2: The Anti-Inflammatory, Nervous System-Supportive Vegan Plate
This section actively rebuilds autonomic function using whole-food fats, coconut oil, and therapeutic foods that restore the copper-vitamin C axis, blood volume, and micronutrient status.
2.1 Embrace Whole-Food Fats and Coconut Oil for Omega-6:3 Balance
Replace all extracted oils with whole-food fat sources and coconut oil. This naturally limits linoleic acid intake, provides stable energy, and eliminates all controversy regarding oil processing and oxidation.
- The Sole Permitted Extracted Oil: Coconut Oil
- Rationale: Coconut oil is a unique saturated fat derived from the fruit of the coconut palm, not a seed. It is composed predominantly of stable saturated fatty acids that do not participate in the peroxidative lipid cascades driven by omega-6 linoleic acid. It provides medium-chain triglycerides (MCTs) that are easily metabolized for energy and have not been implicated in the neuroinflammatory pathways relevant to dysautonomia.
- Use: For all sautéing, roasting, and baking needs.
- Daily Whole-Food Fats:
- Fresh Avocado (Not Oil): Eat whole, fresh avocados for monounsaturated fat, potassium, and magnesium in their complete whole-food matrix.
- Whole Olives (Not Oil): Consume whole, traditionally cured olives as a sodium-rich, whole-food fat source.
- Raw Nuts and Seeds: Consume raw, soaked nuts and seeds (sunflower seeds, pumpkin seeds, sesame seeds, cashews, walnuts) in their whole form.
- Daily, Concentrated Omega-3 from Algal Oil (Capsule): To actively reset the omega-6:3 ratio, a daily algal oil supplement in capsule form is essential, providing 1-2 grams of combined DHA/EPA. This is a therapeutic supplement, not a culinary oil (DiNicolantonio & O’Keefe, 2018).
2.2 A Vegan, High-Sodium, Volume-Expanding Diet
This directly counteracts hypovolemia and renal sodium wasting, which are often worsened by low-carb diets (Borer, 2013). This is not a low-salt diet.
- Aggressive Sodium Loading: Use generous amounts of natural sea salt or pink Himalayan salt on all food. Drink salted vegetable broths daily. A typical goal is 4-8 grams of sodium per day, added to food and fluids, under medical supervision.
2.3 The Critical Role of Carbohydrates for Cellular Energy Efficiency in Dysautonomia
A strict low-carbohydrate diet is profoundly destabilizing for dysautonomia. This section details why adequate, high-quality carbohydrates are non-negotiable for autonomic recovery, linking directly to the mitochondrial and volume-expansion mechanisms previously established.
- Carbohydrates as the Preferred Fuel for a Compromised Mitochondrion:
The autonomic nervous system has extraordinarily high energy demands. The copper-dependent enzyme Cytochrome c Oxidase (COX), or Complex IV, is often impaired in dysautonomia, reducing mitochondrial efficiency (Matoba et al., 2005). In a state of mitochondrial dysfunction, glucose is the most efficient fuel source. It requires less oxygen per molecule of ATP produced compared to fatty acids (a higher P/O ratio). Forcing a mitochondria-damaged system to rely on beta-oxidation of fats for energy, as occurs on a low-carb or ketogenic diet, is metabolically inefficient and places additional oxidative stress on an already struggling system. - Carbohydrates Drive Sodium Retention and Blood Volume:
As established by Borer (2013), insulin is a primary signal for sodium reabsorption in the kidney. Consuming adequate complex carbohydrates stimulates a healthy, physiological insulin response, which directly signals the kidneys to hold onto sodium and water, expanding plasma volume. A low-carb diet abolishes this signal, inducing natriuresis (sodium wasting) and volume contraction, which is the exact opposite of the therapeutic goal in dysautonomia. - Glycogen as Osmotic Stability:
Each gram of glycogen is stored with 3-4 grams of water. Adequate carbohydrate intake ensures replete glycogen stores in the liver and muscles, providing a stable reservoir of water. This prevents the rapid fluid shifts and volatile blood pressure drops that occur when glycogen-bound water is depleted on a low-carb diet. - Avoiding the Sympathetic Stress of Gluconeogenesis:
When carbohydrate intake is insufficient, the body must maintain blood glucose through hepatic gluconeogenesis. This process is driven by the stress hormones cortisol, epinephrine, and glucagon. For a patient with a hyperadrenergic state, a low-carb diet essentially imposes a chronic pharmacological stress test, continuously elevating the catecholamines that the protocol is trying to stabilize. - Practical Carbohydrate Implementation (The “Energy-Efficiency Plate”):
- Primary Staples: Build each meal around a foundation of gently cooked, mineral-dense, complex carbohydrates: sweet potatoes (with skin), purple potatoes, yuca, quinoa, buckwheat, steel-cut oats, and well-cooked brown rice.
- Preparation for Digestion and Volume: Cook grains and starches with a generous pinch of sea salt and a spoonful of coconut oil. The salt supports the volume-expanding insulin-sodium axis, the coconut oil provides stable energy and slows glucose absorption slightly for a gentler blood sugar curve, and the cooking process ensures easy digestion.
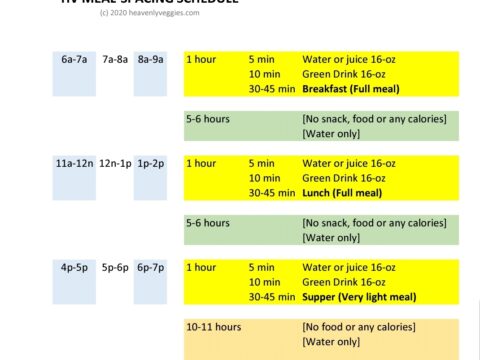
- Meal Timing: Consume 3 balanced meals per day with adequate carbohydrates at each meal to provide a steady stream of glucose for mitochondrial energy and insulin-driven sodium retention, preventing the sympathetic spikes associated with hypoglycemia.
2.4 The Copper-Vitamin C Synergy Meal (The “DBH Restorer”)
Consume one meal daily that specifically combines high-copper, high-vitamin C, high-carbohydrate, and high-magnesium whole vegan foods to restore the two-cofactor system for norepinephrine synthesis, cooked gently in coconut oil.
- The “DBH Restoring” Bowl: A base of steamed quinoa or a baked sweet potato (complex carbohydrate for energy and sodium retention) topped with shiitake mushrooms (copper) and a generous handful of sunflower seeds (copper, magnesium), sautéed gently in coconut oil. Dress with a sauce of whole blended avocado, fresh lemon juice, and sea salt. Served alongside a raw red bell pepper and kiwi salad (vitamin C). This single meal delivers a powerful, synergistic combination of the primary cofactors and energy substrates needed for DBH, PAM, and COX function (Prohaska & Broderius, 1997; Levine et al., 1996).
2.5 Micronutrient Replenishment for Autonomic Resilience
- Magnesium: Best vegan sources include pumpkin seeds, spinach, and Swiss chard. Supplement with magnesium glycinate for its parasympathetic and NMDA-antagonist effects (Sartori et al., 2012).
- Vitamin B12: A sublingual methylcobalamin supplement of 1000-2000 mcg daily is non-negotiable for autonomic nerve myelination (Saperstein et al., 2020).
- Iron: Combine iron-rich foods (lentils, pumpkin seeds) with vitamin C-rich foods in the same meal, cooked in a cast-iron skillet. Aim for a ferritin level >50 µg/L (Jarjour & Jarjour, 2013).
- Liposomal Vitamin C: Supplement with 1000-2000 mg daily in divided doses to support adrenal cortical function and catecholamine synthesis, addressing the depletion caused by chronic stress (Marik, 2020; Padayatty et al., 2003).
Part 3: Lifestyle and Body-Based Practices for ANS Retraining
Nutrition provides the substrate, but the nervous system must be physically retrained.
- The Levine Protocol (Graduated Recumbent Exercise): Begin with recumbent cycling, rowing, or swimming to strengthen the skeletal muscle pump, starting with short durations and progressing very slowly over months.
- Vagus Nerve Activation: Practice daily deep diaphragmatic breathing with an extended exhale (e.g., 4-second inhale, 8-second exhale) and brief cold water face immersion to trigger the mammalian dive reflex.
- Circadian Stability: Maintain a strict sleep-wake schedule, ideally with the head of the bed slightly elevated (4-6 inches) to support morning blood pressure.
Summary: The Daily Recovery Checklist
| Strategy | Daily Actionable Goal | Target Mechanism |
|---|---|---|
| Oil Elimination | Zero consumption of any extracted oil except coconut oil. Read every label. | Halt the substrate for neurotoxic lipid peroxidation (4-HNE); eliminate all controversial oil sources. |
| Whole-Food Fats & Omega-3 | 1-2g DHA/EPA from algal oil capsules; whole avocado, olives, raw soaked nuts/seeds; coconut oil for cooking. | Actively reset the omega-6:3 ratio; provide stable, non-inflammatory whole-food energy. |
| Carbohydrates for Energy Efficiency | Base every meal on sweet potatoes, quinoa, buckwheat, or oats, cooked with salt and coconut oil. | Provide efficient glucose fuel for impaired mitochondria (COX); drive insulin-mediated sodium/volume retention; prevent gluconeogenic sympathetic stress. |
| Hydration & Volume | 2-3 liters of water with sea salt; daily salted broth; whole olives. | Expand blood volume; counteract hypovolemia. |
| Copper-Vitamin C Plate | A “DBH Restoring” bowl with carbohydrate base, shiitake, sunflower seeds, avocado-lemon dressing, bell pepper, and kiwi. | Replenish copper & ascorbate cofactors; restore DBH, PAM, & COX activity. |
| Adrenal Support | Licorice/tulsi tea (if tolerated); 1000-2000mg liposomal Vitamin C. | Support cortical steroidogenesis; quench adrenal oxidative stress. |
| Parasympathetic Training | 10 min of 4:8 breathing; morning cold water face immersion. | Activate vagus nerve; lower sympathetic burst frequency. |
| Nutrient Insurance | Sublingual methylcobalamin (B12); Mg glycinate; cook in cast iron. | Support nerve myelination; calm CNS; optimize ferritin. |
| Strategic Movement | Recumbent cardio (rowing/swimming) for 20-30 min. | Strengthen muscle pump; improve vascular tone without orthostasis. |
This revised protocol is designed as a systematic, root-cause approach. It emphasizes that adequate complex carbohydrates are not optional but essential for providing efficient cellular energy to a mitochondria-damaged autonomic nervous system, driving the blood volume expansion necessary for hemodynamic stability, and preventing the sympathetic stress response of a low-carbohydrate state.
Scientific References
- Benowitz NL. Clinical pharmacology of caffeine. Annual Review of Medicine. 1990;41:277-288.
- Borer KT. Counterregulation of insulin by glucagon and epinephrine during high-intensity exercise and starvation. Sports Medicine. 2013;43(3):219-229.
- Bousquet-Moore D, et al. Interactions of copper with the peptidylglycine α-amidating monooxygenase (PAM) and the subsequent effects on neuropeptide production and function. Cellular and Molecular Life Sciences. 2010;67(16):2679-2692.
- DiNicolantonio JJ, O’Keefe JH. Omega-6 vegetable oils as a driver of coronary heart disease: the oxidized linoleic acid hypothesis. Open Heart. 2018;5(2):e000898.
- Jarjour IT, Jarjour LK. Low iron storage and postural orthostatic tachycardia syndrome in adolescents. Pediatric Neurology. 2013;48(3):218-221.
- Kumar N. Copper deficiency myelopathy (human swayback). Mayo Clinic Proceedings. 2006;81(10):1371-1384.
- Levine M, et al. Vitamin C pharmacokinetics in healthy volunteers: evidence for a recommended dietary allowance. Proceedings of the National Academy of Sciences. 1996;93(8):3704-3709.
- Marik PE. Vitamin C: an essential “stress hormone” during sepsis. Journal of Thoracic Disease. 2020;12(Suppl 1):S84-S88.
- Matoba S, et al. Copper deficiency leads to a mitochondrial dysfunction via impaired complex IV activity in murine hearts. Biochemical and Biophysical Research Communications. 2005;337(2):445-450.
- Padayatty SJ, et al. Vitamin C as an antioxidant: evaluation of its role in disease prevention. Journal of the American College of Nutrition. 2003;22(1):18-35.
- Patak P, et al. Vitamin C is an important cofactor for both adrenal cortex and adrenal medulla. Endocrine Research. 2004;30(4):871-875.
- Prohaska JR, Broderius M. Copper deficiency alters rat dopamine-β-monooxygenase activity and mRNA abundance. The Journal of Nutrition. 1997;127(6):1079-1083.
- Saperstein DS, et al. The evaluation and management of autonomic dysfunction. Neurologic Clinics. 2020;38(4):837-854.
- Sartori SB, et al. Magnesium deficiency induces anxiety and HPA axis dysregulation: modulation by therapeutic drug treatment. Neuropharmacology. 2012;62(1):304-312.
- Smith-Mungo LI, Kagan HM. Lysyl oxidase: properties, regulation and multiple functions in biology. Matrix Biology. 1998;16(7):387-398.
- Wimalawansa SJ. Vitamin D and cardiovascular system: A review of mechanisms. Nutrients. 2019;11(11):2749.
The following bibliography provides the complete scientific foundation for the mechanistic rationale and the practical nutritional and lifestyle interventions detailed in the dysautonomia recovery protocol above.
Scientific Rationale for the Dysautonomia Recovery Protocol
- Benowitz NL. Clinical pharmacology of caffeine. Annual Review of Medicine. 1990;41:277-288.
- Summary: A foundational review of caffeine’s dose-dependent cardiovascular and autonomic effects, including adenosine receptor antagonism, catecholamine release, and diuretic properties.
- Borer KT. Counterregulation of insulin by glucagon and epinephrine during high-intensity exercise and starvation. Sports Medicine. 2013;43(3):219-229.
- Summary: Explains the neuroendocrine axis where low insulin and glucose availability trigger a compensatory epinephrine/sympathetic surge and renal sodium wasting, directly relevant to the destabilizing effects of low-carbohydrate diets.
- Bousquet-Moore D, Mains RE, Eipper BA. Interactions of copper with the peptidylglycine α-amidating monooxygenase (PAM) and the subsequent effects on neuropeptide production and function. Cellular and Molecular Life Sciences. 2010;67(16):2679-2692.
- Summary: A comprehensive review detailing how the copper-dependent enzyme PAM is essential for activating neuropeptides including VIP, CCK, and NPY, and how copper deficiency impairs vagal tone and autonomic regulation.
- DiNicolantonio JJ, O’Keefe JH. Omega-6 vegetable oils as a driver of coronary heart disease: the oxidized linoleic acid hypothesis. Open Heart. 2018;5(2):e000898.
- Summary: Details how oxidized linoleic acid metabolites from industrial seed oils drive vascular and cellular inflammation, with direct applicability to neurovascular autoregulation and small fiber neuropathy.
- Jarjour IT, Jarjour LK. Low iron storage and postural orthostatic tachycardia syndrome in adolescents. Pediatric Neurology. 2013;48(3):218-221.
- Summary: A study demonstrating a significant correlation between low ferritin levels and POTS symptoms, with clinical improvement upon iron repletion.
- Kumar N. Copper deficiency myelopathy (human swayback). Mayo Clinic Proceedings. 2006;81(10):1371-1384.
- Summary: A seminal clinical review describing the neurological and autonomic manifestations of acquired copper deficiency, including the mechanisms of malabsorption and biliary excretion.
- Levine M, Conry-Cantilena C, Wang Y, et al. Vitamin C pharmacokinetics in healthy volunteers: evidence for a recommended dietary allowance. Proceedings of the National Academy of Sciences. 1996;93(8):3704-3709.
- Summary: A landmark pharmacokinetic study establishing vitamin C’s role as an essential cofactor for dopamine-β-hydroxylase and its concentration-dependent bioavailability in human tissues.
- Marik PE. Vitamin C: an essential “stress hormone” during sepsis. Journal of Thoracic Disease. 2020;12(Suppl 1):S84-S88.
- Summary: A clinical review highlighting vitamin C’s critical, rapidly depleted role as a cofactor for catecholamine synthesis and adrenal steroidogenesis during physiological stress.
- Matoba S, Tatsumi T, Keira N, et al. Copper deficiency leads to a mitochondrial dysfunction via impaired complex IV activity in murine hearts. Biochemical and Biophysical Research Communications. 2005;337(2):445-450.
- Summary: An animal study demonstrating that dietary copper deficiency directly impairs cardiac mitochondrial energy production through reduced cytochrome c oxidase (Complex IV) activity.
- Padayatty SJ, Katz A, Wang Y, et al. Vitamin C as an antioxidant: evaluation of its role in disease prevention. Journal of the American College of Nutrition. 2003;22(1):18-35.
- Summary: A comprehensive review of vitamin C’s pharmacokinetics, tissue distribution, and its concentrated role in the adrenal glands as both an antioxidant and enzymatic cofactor.
- Patak P, Willenberg HS, Bornstein SR. Vitamin C is an important cofactor for both adrenal cortex and adrenal medulla. Endocrine Research. 2004;30(4):871-875.
- Summary: Details the dual role of ascorbate in the adrenal gland: as a cofactor for catecholamine synthesis in the medulla and for steroidogenesis and antioxidant protection in the cortex.
- Prohaska JR, Broderius M. Copper deficiency alters rat dopamine-β-monooxygenase activity and mRNA abundance. The Journal of Nutrition. 1997;127(6):1079-1083.
- Summary: An animal study directly demonstrating that dietary copper deficiency significantly reduces DBH enzyme activity, establishing the direct biochemical link between copper status and norepinephrine synthesis.
- Saperstein DS, Levine TD, Farhad K, et al. The evaluation and management of autonomic dysfunction. Neurologic Clinics. 2020;38(4):837-854.
- Summary: A clinical review detailing the role of B12 deficiency and other metabolic neuropathies as reversible causes of autonomic failure, and the comprehensive diagnostic approach to dysautonomia.
- Sartori SB, Whittle N, Hetzenauer A, Singewald N. Magnesium deficiency induces anxiety and HPA axis dysregulation: modulation by therapeutic drug treatment. Neuropharmacology. 2012;62(1):304-312.
- Summary: An animal model study demonstrating how dietary magnesium deficiency directly causes neuronal dysregulation, a hyperadrenergic state, and HPA axis dysfunction.
- Smith-Mungo LI, Kagan HM. Lysyl oxidase: properties, regulation and multiple functions in biology. Matrix Biology. 1998;16(7):387-398.
- Summary: A foundational review on the copper-dependent enzyme lysyl oxidase, detailing its mechanism of action and its critical role in collagen and elastin cross-linking for vascular wall integrity.
- Wimalawansa SJ. Vitamin D and cardiovascular system: A review of mechanisms. Nutrients. 2019;11(11):2749.
- Summary: A review discussing the non-skeletal functions of Vitamin D, including its role in autonomic tone, cardiovascular regulation, and immune modulation.
![]()